
The first and only
KA-optimized implant
To potentially further improve KA results and ultimately patient satisfaction, Medacta has developed GMK SpheriKA, the first and only KA-optimized implant.
GMK SpheriKA was developed starting from the strong heritage of GMK Sphere, with a particular focus on the anterior aspect of the femur.

Kinematic Alignment is a technique that resurfaces the knee to its pre-arthritic state. By doing so, it restores the native Joint Line Orientation, pre-arthritic alignment, and knee kinematic axes, ultimately leading to native soft tissue laxity and normal kinematic profile. In recent years Kinematic Alignment has been shown to provide better functional scores and patient outcomes in different comparative studies 1,3.
However, femoral implants currently on the market are mainly designed for the Mechanical Alignment (MA) technique. This could potentially represent a limitation to the KA technique 4,5.


Medacta's GMK Sphere has been proven to be a particularly suitable implant for KA 6-10, as it provides stability with its Ball-in-Socket design, while allowing patient-specific kinematic patterns with its unconstrained lateral compartment 11-14.
When combined with the KA technique, the GMK Sphere has been shown to provide better functional scores and improve patient outcomes compared to other designs 6-10.

Patients who receive a total knee replacement prefer a feeling of “stability”17.
Over the years, GMK Sphere has been proven to:
• Provide functional stability while allowing for patient-specific kinematics11-14.
• Improve patient satisfaction even when compared to other implant designs18.
MEDIAL BALL-IN-SOCKET
A 1:1 congruent medial compartment provides high functional stability during the most demanding activities throughout the whole Range of Motion12,15,16 .
UNCONSTRAINED LATERAL COMPARTMENT
Ensuring complete freedom of rollback and rotation to accommodate the best pattern of kinematic motion for each patient16.
MEDIAL CONGRUENT IS NOT BALL-IN-SOCKET
Only a true Ball-in-Socket design provides full conformity between femur and insert throughout the range of motion, maximizing antero-posterior stability and allowing for an unconstrained lateral compartment 11-14.


The GMK SpheriKA design is based on an extensive anthropometric research project using the MyBody database* containing more than 150,000 CT and MRI scans.
This study was conducted to identify the anterior aspect of the femur and potentially correlate it with different phenotypes or demographic parameters.
The result of the analysis is in line with other clinical publications, indicating that there is a high degree of variability in the native trochlea orientation among patients 19.
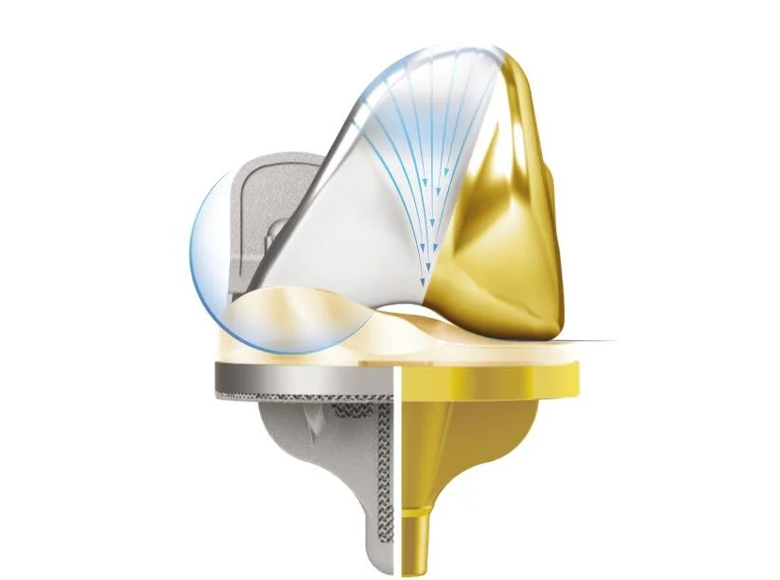
FUNNEL-DESIGNED TROCHLEA GROOVE
The groove is open proximally to accommodate a wider range of Q-angles (up to 20° of valgus), becoming more constraining at higher degrees of knee flexion.
OPTIMIZED BONE COVERAGE FOR THE KA TECHNIQUE
The antero-lateral ridge is designed to better accomodate the valgus femoral cuts applied in the KA technique and reduce the risk of bony uncoverage.

An extensive anthropometric research performed in the MyBody database* containing more than 150,000 CT and MRI scans of knees has led to the validation of the following19:
The combination of 13 femoral sizes and inserts with 1 mm increments allows the surgeon to “fine tune” ligament balance and improve stability throughout the range of motion.

MectaGrip
Highly porous titanium plasma sprayed coating designed to achieve primary stability and secondary fixation19.
SensiTiN
Ceramic-like coating designed to reduce the release of metal ions from the implant19.
E-CROSS
Vitamin E highly crosslinked UHMWPE with improved oxidation and wear resistance19.
13 sizes
Anatomical: left and right
Cemented: 0.5 mm deep pockets
Material: Cobalt-Chrome (Co-Cr-Mo ISO 5832-4)

Material: Cobalt-Chrome (Co-Cr-Mo ISO 5832-4) + SensiTiN coating

Materials: Co28-Cr6-Mo - ISO 5832-4 + Titanium coating - ASTM F1580 with Hydroxyapatite - ASTM F1185

6 sizes
Anatomical: left and right
7 levels of thickness (10, 11, 12, 13, 14, 17, 20 mm)
Machined Ultra High Molecular Weight Polyethylene (UHMWPE ISO 5834-2)

E-CROSS (Vitamin E Highly Crosslinked UHMWPE)

6 sizes
Anatomical: left and right
5 levels of thickness (10, 11, 12, 13, 14 mm)
Machined Ultra High Molecular Weight Polyethylene (UHMWPE ISO 5834-2)

E-CROSS (Vitamin E Highly Crosslinked UHMWPE)

6 sizes
Anatomical: left and right
Cemented: 0.5 mm deep pockets
Material: Cobalt-Chrome (Co-Cr-Mo ISO 5832-4)

Material: Cobalt-Chrome (Co-Cr-Mo ISO 5832-4) + SensiTiN coating

Anatomical shape
4 sizes
Machined Ultra High Molecular Weight Polyethylene (UHMWPE ISO 5834-2)
Cemented
Three fixation pegs

E-CROSS (Vitamin E Highly Crosslinked UHMWPE)

Diameter x length: 11x 30 mm and 11 x 65 mm
Cemented

GMK SpheriKA is supported by advanced enabling technologies, part of Medacta's MySolutions Personalized Ecosystem and supporting both MA and KA alignments.
.jpg)
MyKnee is a set of patient-specific blocks, allowing the surgeon to reproduce their 3D preoperative planning, based on CT or MRI images of the patient’s knee.
Discover more >
.jpg)
NextAR Knee delivers intraoperative guidance within the surgeon’s operative field, through a compact disposable tracking system and augmented reality glasses.
Discover more >

GMK Efficiency is a complete single-use instrument solution designed to simplify inventory management, back table setup, and reduce facilities’ reliance on decontamination practices for metal instrumentation. GMK Efficiency can be used as a stand-alone solution or in combination with MyKnee or NextAR.
Discover more >

A complete and efficient system
GMK SpheriKA is supported by MyKA, a comprehensive platform for Kinematic Alignment, that features dedicated instruments and technologies and a tailored M.O.R.E. Education Program. Medacta has been a pioneer of this technique, in line with its pillar of responsible innovation to improve patient satisfaction.
[1] Lee, Yong Seuk, et al. "Kinematic alignment is a possible alternative to mechanical alignment in total knee arthroplasty." Knee Surgery, Sports Traumatology, Arthroscopy 25 (2017): 3467-3479.
[2] Courtney, P. Maxwell, and Gwo-Chin Lee. "Early outcomes of kinematic alignment in primary total knee arthroplasty: a meta-analysis of the literature." The Journal of arthroplasty 32.6 (2017): 2028-2032.
[3] Blakeney, William, et al. "Kinematic alignment in total knee arthroplasty better reproduces normal gait than mechanical alignment." Knee Surgery, Sports Traumatology, Arthroscopy 27 (2019): 1410-1417.
[4] Rosa, Sergio Barroso, Kaushik Hazratwala, and Matthew PR Wilkinson. "Mismatch between trochlear coronal alignment of arthritic knees and currently available prosthesis: a morphological analysis of 4116 knees and 45 implant designs." Knee Surgery, Sports Traumatology, Arthroscopy 31.8 (2023): 3116-3123.
[5] Wang, Zhiwei, et al. "Undercoverage of lateral trochlear resection is correlated with the tibiofemoral alignment parameters in kinematically aligned TKA: A retrospective clinical study." BMC Musculoskeletal Disorders 22.1 (2021): 1-9. [6] Jeremić, Dragan V., et al. "Short-term follow-up of kinematically vs. mechanically aligned total knee arthroplasty with medial pivot components: a case-control study." Orthopaedics & Traumatology: Surgery & Research 106.5 (2020): 921-927.
[6] Jeremić, Dragan V., et al. "Short-term follow-up of kinematically vs. mechanically aligned total knee arthroplasty with medial pivot components: a case-control study." Orthopaedics & Traumatology: Surgery & Research 106.5 (2020): 921-927.
[7] Ziv, Yaron Bar, et al. "Patients undergoing staged bilateral knee arthroplasty are less aware of their kinematic aligned knee compared to their mechanical knee." Journal of Orthopaedics 23 (2021): 155-159.
[8] Scott, David F., and Celeste G. Gray. "Outcomes are better with a medial-stabilized vs a posterior-stabilized total knee implanted with kinematic alignment." The Journal of Arthroplasty 37.8 (2022): S852-S858
[9] Scott, David F., and Amy A. Hellie. "Mid-Flexion, Anteroposterior Stability of Total Knee Replacement Implanted with Kinematic Alignment: A Randomized, Quantitative Radiographic Laxity Study with Posterior-Stabilized and Medial-Stabilized Implants." JBJS 105.1 (2023): 9-19.
[10] JONES, Brett K.; CARLSON, Brian J.; SCOTT, David F. Better flexion and early recovery with medial-stabilized vs single-radius total knee arthroplasty with kinematic alignment: Two-year clinical results. The Knee, 2023, 43: 217-223
[11] Scott, G., et al. "Can a total knee arthroplasty be both rotationally unconstrained and anteroposteriorly stabilised?: A pulsed fluoroscopic investigation." Bone & Joint Research 5.3 (2016): 80-86.
[12] Morra EA, Greenwald AS “Simulated kinematic performance of The GMK-Sphere Total Knee Design During A Stand to Squat Activity” Study Report 2013.
[13] Steinbrück, Arnd, et al. "Femorotibial kinematics and load patterns after total knee arthroplasty: an in vitro comparison of posterior-stabilized versus medial-stabilized design." Clinical Biomechanics 33 (2016): 42-48.
[14] Schütz, Pascal, et al. "Kinematic evaluation of the GMK sphere implant during gait activities: a dynamic videofluoroscopy study." Journal of Orthopaedic Research® 37.11 (2019): 2337-2347.
[15] Hossain F et al. “Knee arthroplasty with a medially conforming ballandsocket tibiofemoral articulation provides better function”, Clin Orthop Relat Res. 2011 Jan;469(1):55-63.
[16] Banks S et al, “In Vivo Kinematics of a Medially Conforming & Rotationally Unconstrained TKA Design”, Podium presentation
at the 27th Annual Meeting of the International Society for Technology in Arthroplasty, Kyoto, Japan, September 25-27, 2014.
[17] Pritchett JW “Patients Prefer A Bicruciate-Retaining or the Medial Pivot Total Knee Prosthesis”, The Journal of Arthroplasty, 2011.
[18] Dowsey, Michelle M., et al. "A randomized controlled trial comparing a medial stabilized total knee prosthesis to a cruciate retaining and posterior stabilized design: a report of the clinical and functional outcomes following total knee replacement." The Journal of Arthroplasty 35.6 (2020): 1583-1590.
[19] Data on file: Medacta.
* The CT and MRI scans contained in the “MyBody” database are anonymous and do not permit in any way the identification of patients. Medacta recognizes the importance of personal data protection and considers that preserving the confidentiality of personal data is one of the main objectives of its activity, in compliance with any applicable privacy law and regulation.






